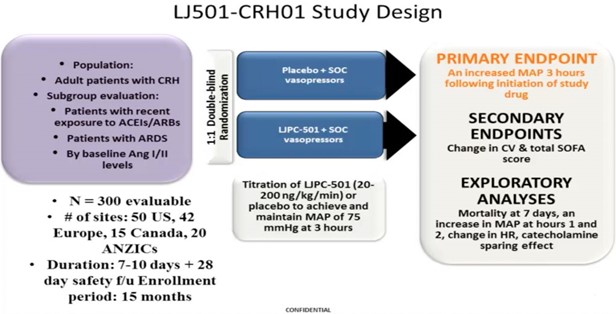
Mastering Vasopressor Management Rules of Critical Care 1. Defend the blood pressure “True” hypotension is an emergencyMAP<65 needs attention IMMEDIATELYHypotension →Decreased DBP → Decreased coronary blood flow → Cardiac ischemia → Decreased CO → Hypotension (repeat)Short durations hurt brain, kidneys, heart Longer durations of hypotension = worse outcomesPush dose, immediate fluids, etc.FIX IT! 2. You MUST diagnose shock Always identify which type of shock!Stabilize/Defend BPAssessment of CO → Diagnose shock typeVolume trial → Look for CO improvement The choice of vasopressors is not always clear The case for Vasopressin>NE: VASST trialsAre both studies underpowered? Is steroids+Vaso the magic solution for the truly sick?No consensus solutionThe comparison of NE to Dopa(SOAP II group)Poorly dosed Dopa in the comparison group (not studying the physiological rationale)NE maybe better for you (for cardiogenic shock)Hypotension is due to a lack of catecholamines (just as HTN is due to an overabundance of them) Alternative vasopressors: What is in the pipeline? Selepressin Vasopressin targets V1a, V1b for vasoconstrictionAlso targets Oxytocin and V2→ fluid overload and microvascular thrombosis Selepressin is a selective V1a agonist → targeted vasoconstrictionImproves free water clearance (lacks V2 targeting) → less lung injury/less lung edemaLess vascular leak(typical with Vasopressin)Angiotensin II (Ang II)First trial: 1961, then disappearedExample: Distributive shock, s/p resuscitation, has INCREASED blood flow to kidneys → intraglomerular hypotension and AKITreatment with Ang II leads to improvementsNE leads to AFFERENT vasoconstrictionAng II→ EFFERENT vasoconstriction (recruits capillary beds) ATHOS trialLow doses of Ang II can causecatecholamine sparing2 outliers had HYPERtension (due to ARDS?) SEVERE ARDS causes Ang II deficiencyPulmonary capillary endothelium damage can restrict conversion of Ang I to Ang IIAng II Pilot data conclusionsIV Ang II has a role as a rescue vasopressorIV Ang II may bemore useful in ARDS patientsCurrently undergoing a Phase III registration trial for Ang II as a vasopressorFirst FDA trial for a drug AS a vasopressor